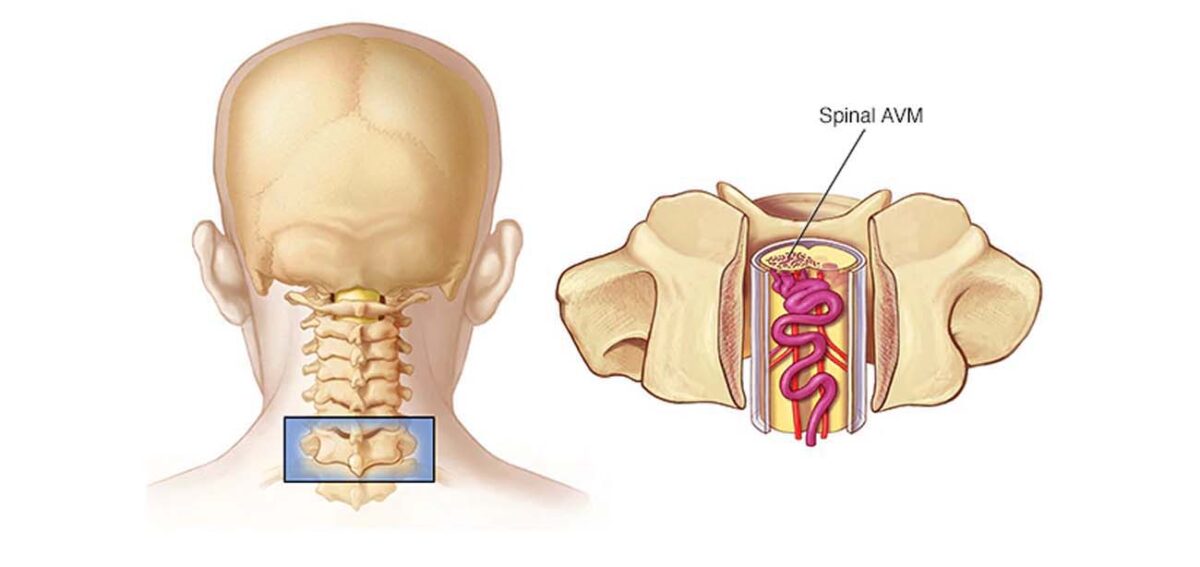
Arteriovenous malformation (AVM) is a tangle of abnormal blood vessels connecting veins and arteries. When they occur in or around the spinal cord they are called Spinal AVM.
Typically, blood flows from the heart to the arteries, which get smaller until they turn into capillaries. Nutrients and oxygen exchange takes place in the capillaries. The blood then passes from capillaries to your heart through veins.
But in the AVM’s, arteries directly connect to veins, without capillaries in between, and form a knot of blood vessels. This creates an area of high pressure. The veins cannot take this pressure and enlarge and bulge to accept extra blood coming at high pressure. In this process they may exhibit pressure symptoms on the spinal cord resulting in disabilities or may bleed causing serious complications.
Spinal AVMs can be seen at any age depending upon their type. Typically when they are inside the spinal cord they present early and are commonly seen in the young children, and when they are around the spinal cord they present in the adults or older age group.
Symptoms
Manifestation of spinal AVM may be different in different patients depending on its location and size. While some may not have noticeable symptoms, others may have life-threatening symptoms.
When present, some common symptoms include:
- Tingling or, numbness, in your legs or arms.
- Problems with climbing stairs or walking.
- Weakness on one or both the sides of your body.
- Difficulty in passing urine or stools.
If left unattended, spinal AVM may cause the following symptoms:
- Lack of sensation in your legs
- Paralysis of arms/legs.
- Difficulty moving your bowels or urinating.
Diagnosis
Spinal malformations can be challenging to diagnose as their signs and symptoms resemble other spinal disorders, such as spinal stenosis or other spinal infections.
Here are some tests that can help your doctor diagnose this condition:
- Magnetic resonance imaging (MRI): it frequently raises the suspicion of underlying AVM. It also helps in assessing the damage caused to the spinal cord or if there is any bleeding due to AVM.
- Digital Substraction Angiography (DSA): this is gold standard for spinal AVM diagnosis. Spinal angiography (DSA) also aids in identifying the blood vessels supplying the malformation, type of AVM and thus planning the right treatment approach.
Spinal Vascular Malformations Treatment
Treatment strategies and outcomes depend on the location, size, and blood flow to your spinal AVM, overall health, and neurological examination.
The primary goal of treatment is to lower the risk of bleeding and prevent or stop the progression of disability.
Pain-reliving medicines may reduce symptoms such as stiffness and back pain, but most patients will gradually need surgery.
Surgery
It helps in removing a spinal AVM from the surrounding tissues. Some common options include:
Conventional surgery: A surgeon makes an incision to remove the AVM. Care is taken to avoid damage to the spinal cord and its surrounding structures. This type of surgery is done when AVM is located in an area that is easily accessible and fairly small in size. - Endovascular embolization: It is a minimally invasive procedure involving the insertion of a flexible, thin tube (catheter) through a cut in the groin to deliver obstructive materials like glue or onyx into AVM and close the abnormal connection. At present this is the mainstay in the treatment of spinal AVM. Once diagnosed this form of surgery needs to be done at the earliest to prevent the progression of the deficits.
- Radiosurgery: It uses a highly concentrated radiation beam that focuses on the site of AVM with the help of dedicated machines. The radiation beam damages the blood vessels and forms scar tissue that stops the blood flow into the AVM. The procedure is cut-free and painless. Radiosurgery is ideal for smaller, unruptured AVMs. The flip side to this treatment is that the effect of this treatment takes months to year to become evident unlike embolization where the AVM can be blocked right then during the treatment session.
Comments 0