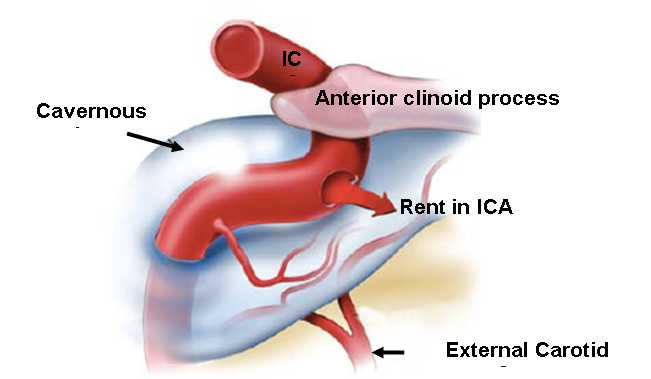
A carotid-cavernous fistula (CCF) is an atypical connection between the carotid artery (or its branches) and the cavernous sinus. The cavernous sinus is a large venous poch located behind your eye that receives blood from the orbit, brain, and pituitary gland. The carotid-cavernous fistula can be direct (high-flow) or indirect (low-flow).
Causes
The causes may be divided into two main types:
- Traumatic (Direct): This may occur after a head injury, which can range from falls to penetrative wounds.
- Spontaneous (Indirect): It may usually occur due to a spontaneous rupture of a cavernous carotid aneurysm. However, this type of fistula can also be due to a congenital abnormal connection between artery and vein that spontaneously opens due to atherosclerotic disease, collagen vascular disease, childbirth, or hypertension.
Symptoms
Direct CCF
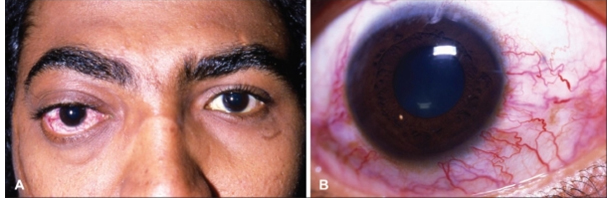
Symptoms usually occur days or weeks after ahead injury. Common symptoms include:
- Chemosis or red-eye syndrome
- Pulsatile exophthalmos or protrusion of the eyeball
- Ocular bruit or blood flow sounds from the eye
- Other symptoms such as double vision or visual loss may also result
Indirect CCF
This type has a gradual onset and milder symptoms. The patient has a chronically red eye, but the ocular bruit is absent.
Instigations
The following tests may help:
CT Angiography
It is a non-invasive imaging investigation to evaluate a suspected CCF. CT angiography can detect exophthalmos, orbital congestion, enlarged superior ophthalmic vein, bulging cavernous sinus, intracranial hemorrhage, or enlargement or cavernous sinus.
Angiography (DSA)
Digital subtraction angiography is a gold standard imaging technique for CCF due to its high resolution. It may help detect the features of CCF, such as enlarged draining veins, shunting from the internal carotid artery to the cavernous sinus, and retrograde flow from the sinus into the ophthalmic veins.
Ultrasound
Doppler ultrasound may show arterialized ophthalmic veins.
Treatment
These fistulas can be managed through endovascular or microvascular neurosurgical techniques. However, the endovascular approach is usually preferred due to low morbidity.
Endovascular Therapy
Direct CCFs were usually managed by sealing the fistula with detachable balloons introduced through the blood vessel while preserving the internal carotid artery. Nowadays, treatment options include coiling of the fistula or placement of a stent through a trans-arterial route.
In cases where the trans-arterial route is ineffective or impossible, platinum coils are introduced through a transvenous approach. This can be done using the femoral route through the inferior petrosal sinus. Alternatively, the procedure can be done surgically through a superior ophthalmic vein.
Indirect CCFs usually resolve on their own. If not, manual carotid compression is the initial option for low-risk CCFs. This can manage about 30% of the indirect CCFs.
In patients where compression is not recommended, such as those with retrograde filling of the cortical venous system, a transvenous or trans arterial approach is used.
Surgical Treatment
This procedure involves a craniotomy and sealing the internal carotid artery proximal and distal to the fistula using clips. The sinus is then occluded with fascia, acrylate glue, or Surgicel to obstruct the blood flow.
The procedure may also involve connecting the external carotid artery to the middle cerebral artery using a vein or artery to prevent stroke.
Comments 0